Critical Care · NGS in Pleural Fluid
When Pleural Fluid Culture Falls Short.
A 145-specimen ICU evaluation found targeted next-generation sequencing detected pathogens in exudative pleural fluid roughly three times more often than standard culture. Here is what the evidence shows, and where it fits.
Source Lopez-Ruiz et al., AJRCCM 2026 (ATS 2026) Cohort AdventHealth ICU · n = 145 Topic Culture-negative pleural infection

CLINICAL CONTEXT
The Clinical Problem
A patient in the ICU has a large pleural effusion. Imaging, inflammatory markers, and the clinical course all point toward infection. The pleural fluid is drained, sent for culture, and the result comes back negative. Antibiotics are already running. What now informs the decision to continue, narrow, or escalate therapy?
This is one of the more common and more frustrating scenarios in critical care. Large pleural effusions are prevalent in ICU patients and contribute to atelectasis, persistent hypoxemia, impaired resolution of pneumonia, and prolonged mechanical ventilation. Thoracentesis with fluid culture and chemistry analysis is meant to settle whether an effusion can be managed conservatively or needs an aggressive intervention such as chest tube thoracostomy and prolonged antibiotics. The problem is that the decision often hinges on culture, and culture in pleural fluid has a low diagnostic yield, frequently reported below 20 percent.⁴
Parapneumonic and complicated pleural effusions are among the most diagnostically opaque infections clinicians manage, and standard pleural fluid culture frequently returns no organism even when the patient is clearly infected. The practical consequence is familiar: broad-spectrum empiric therapy is started, and because there is no organism to de-escalate against, it is often continued well past the point where a target would have allowed a narrower regimen.
A single-center ICU evaluation presented at the American Thoracic Society 2026 International Conference quantifies that gap directly, comparing standard pleural fluid culture with targeted next-generation sequencing on paired specimens (Lopez-Ruiz et al., 2026).
Why Culture Comes Up Short Here
Three mechanisms account for most of the missed organisms in pleural fluid, and they tend to compound one another in the sickest patients.
- Antibiotic suppression. Pleural fluid is rarely sampled before therapy begins; it is usually drained days into an empiric regimen, by which point viable organisms may be too few to grow.
- Biology of the organisms themselves. Many of the pathogens that drive parapneumonic infection, including anaerobes, oral flora, Mycoplasma, and other fastidious or atypical bacteria, grow poorly or not at all on standard pleural fluid culture panels.
- Polymicrobial complexity. Empyema and complicated parapneumonic effusions are often polymicrobial, and culture tends to report only the dominant aerobe, leaving the rest of the picture unresolved.
Each of these is a reason culture can be negative or incomplete in a patient who is unquestionably infected. A method that does not depend on growth, and that reads bacterial and fungal DNA directly from the specimen, is positioned to recover signal in exactly these situations. That is the hypothesis the Lopez-Ruiz evaluation tested.
THE EVIDENCE
The Evaluation
The investigators performed a single-center retrospective evaluation of 145 paired pleural fluid specimens collected at AdventHealth between January 2020 and February 2025. Each specimen underwent both standard fluid culture and targeted NGS, ordered through MicroGenDX. The NGS workflow combined a limited quantitative PCR panel with 16S rRNA gene sequencing for bacteria and ITS region sequencing for fungi. Effusions were classified as transudates or exudates by Light criteria, and the diagnostic-performance analysis was restricted to exudates, which accounted for 92 percent of the cohort. Because every specimen was tested by both methods, the comparison is matched rather than drawn from separate populations, which strengthens the head-to-head reading within this cohort.
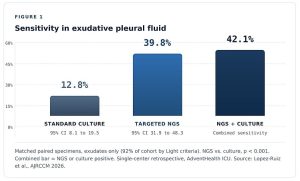
Figure 1. Sensitivity in exudative pleural fluid. Matched paired specimens, exudates only (92% of cohort by Light criteria). NGS vs. culture, p < 0.001. Source: Lopez-Ruiz et al., AJRCCM 2026.
Sensitivity in Exudates
In exudative pleural fluid, standard culture sensitivity was 12.8 percent (95% CI: 8.1 to 19.5). Targeted NGS sensitivity was 39.8 percent (95% CI: 31.9 to 48.3). The difference was statistically significant (p < 0.001). In practical terms, NGS detected a pathogen roughly three times as often as culture in the same specimens. Combining NGS with culture raised sensitivity to 42.1 percent, reflecting the small number of culture-positive specimens NGS did not capture.
Specificity was 100 percent for both methods (95% CI: 75.8 to 100), with no false positives observed among transudates. That detail matters for interpretation: the sensitivity gain did not come at the cost of spurious positives in fluid that was not infected. A positive NGS result in this cohort behaved as a real signal rather than noise.
The Antibiotic-Exposed Subset
Pleural fluid is rarely sampled before antibiotics start. It is usually drained days into empiric therapy, and prior antibiotic exposure is one of the best-understood reasons culture yield collapses. The evaluation looked at this directly.
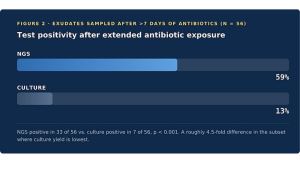
Figure 2. Test positivity after extended antibiotic exposure. Exudates sampled after >7 days of antibiotics (n = 56). NGS positive in 33 of 56 vs. culture positive in 7 of 56, p < 0.001.
Among exudates sampled after more than seven days of antibiotics (n = 56), culture was positive in 13 percent (7 of 56), while NGS was positive in 59 percent (33 of 56), again at p < 0.001. This is the subset where the diagnostic gap matters most: these are precisely the patients in whom culture is least likely to help and in whom the temptation to continue broad coverage indefinitely – with no organism to target or de-escalate against – is strongest.
Concordance and Culture-Negative Yield
Two further findings speak to how NGS would sit alongside culture rather than replace it. Among culture-positive exudates, NGS recovered 84 percent (16 of 19) of the organisms culture identified, so adjunctive use did not come at the expense of losing organisms culture would have found. And NGS detected at least one organism in 74 percent (39 of 53) of culture-negative exudates, expanding the diagnostic picture in exactly the cases where culture had gone silent.
Key Findings · exudates, paired specimens

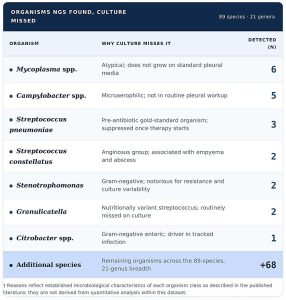
Across the cohort, NGS detected 89 species across 21 genera that culture did not, including organisms that grow poorly or not at all on standard pleural panels.
Organisms NGS Found, Culture Missed · 89 species, 21 genera
CLINICAL APPLICATION
What This Means at the Bedside
The clinical value here is not abstract sensitivity. It is the ability to put a name to an infection that culture has left unnamed, during a critical period where proper microbial identification can substantially alter management and outcomes. Several scenarios stand out.
- Suspected parapneumonic effusion When imaging and the clinical picture support infection but cultures are negative or pending.
- Active or recent antibiotics Culture positivity was 13% in the antibiotic-exposed subset versus 59% for NGS – a roughly 4.5-fold
- Anaerobes or fastidious organisms suspected Oral flora, anaerobic empyema, Mycoplasma, atypical bacteria that grow poorly on standard panels.
- Stewardship-driven decisions Identification supports both narrowing therapy and confirming coverage of a fastidious organism the original regimen might have missed.
- Suspected polymicrobial infection Complicated empyema and tracking effusions; relative abundance reporting supports more targeted therapy.
- Pre-surgical workup When pleural drainage or thoracic surgery is anticipated and organism identification would change peri-operative antibiotics.
A Concrete Workflow
Day five of vancomycin and piperacillin-tazobactam. Culture negative. Markers not improving.
Under a culture-only pathway, the team has no organism and little basis for changing course, so coverage usually continues unchanged. With adjunctive NGS, a species-level identification in the 24-to-48-hour window can convert that stalemate into a decision: a susceptible target supports narrowing, a fastidious organism outside the current spectrum supports a deliberate change, and a credible negative supports reconsidering whether the effusion is infected at all.
Two caveats keep the reading honest. This is a single-center retrospective evaluation, and even with the NGS advantage, absolute sensitivity in exudates was 39.8 percent, so a negative result does not exclude infection. NGS is positioned here as adjunctive to culture, not a replacement for it, and clinical judgment remainsthe arbiter.
THE REPORT
Where MicroGenDX Fits
The targeted NGS used in this evaluation is the MicroGenDX workflow for pleural fluid. A single submission returns the results below.
Species-level via 16S rRNA and ITS: Bacterial 16S rRNA sequencing for prokaryotes and ITS region sequencing for fungi, returned in one workflow.
Antimicrobial resistance gene panel: Detection of clinically significant resistance genes to support targeted therapy and stewardship decisions.
Relative abundance reporting: Polymicrobial specimens reported with relative abundance per organism to help prioritize therapy in mixed infections.
Rapid Turnaround: qPCR and NGS results typically available within 24 to 48 hours from sample receipt.
Testing is performed in a CAP-accredited, CLIA-certified, CLEP-permitted (NYS DOH) laboratory, and every report is reviewed and signed before release. Accepted specimens include pleural fluid, BAL fluid, and swabs, with a minimum testing volume of 2 cc. Peer-to-peer consultation with a MicroGenDX PhD scientist or a practicing physician in the relevant specialty is available on request.
References
- Lopez-Ruiz A, Sniffen JC, Butt TS, Tipton CD, Sniffen K, Ancira J, Patel M, Cearras M, Gleason B, Carrillo MC. Evaluation of Targeted Next-Generation Sequencing Versus Standard Culture for Microbial Detection in Pleural Effusions. Am J Respir Crit Care Med. 2026;212(Suppl 1):aamag162.6017. Presented at the American Thoracic Society International Conference, May 2026, Orlando, FL. DOI: 10.1093/ajrccm/aamag162.6017.
- Babar HSA, et al. Pleural fluid next-generation sequencing case literature. Pathogens. 2024;13(2):165. PMID: 38392903.
- Tipton CD, et al. Targeted NGS analytical validation (16S rRNA and ITS sequencing in synovial fluid; methodology reference). Front Microbiol. 2026. DOI: 10.3389/fmicb.2026.1816780.
- Bedawi EO, Ricciardi S, Hassan M, et al. ERS/ESTS statement on the management of pleural infection in adults. Eur Respir J. 2023;61(2):2201062. DOI: 10.1183/13993003.01062-2022.
For U.S. healthcare professionals only.